The Science
Stephen Porges’ polyvagal theory is the most important piece of neuroscience for understanding why regulation is hard, why willpower fails, and why the path to change runs through the body rather than the mind.
The classical model of the autonomic nervous system described two opposing systems: sympathetic (fight/flight — activating) and parasympathetic (rest/digest — calming). The polyvagal model shows this is incomplete. There are not two states. There are three, and they are hierarchical.
The Three-Zone Hierarchy
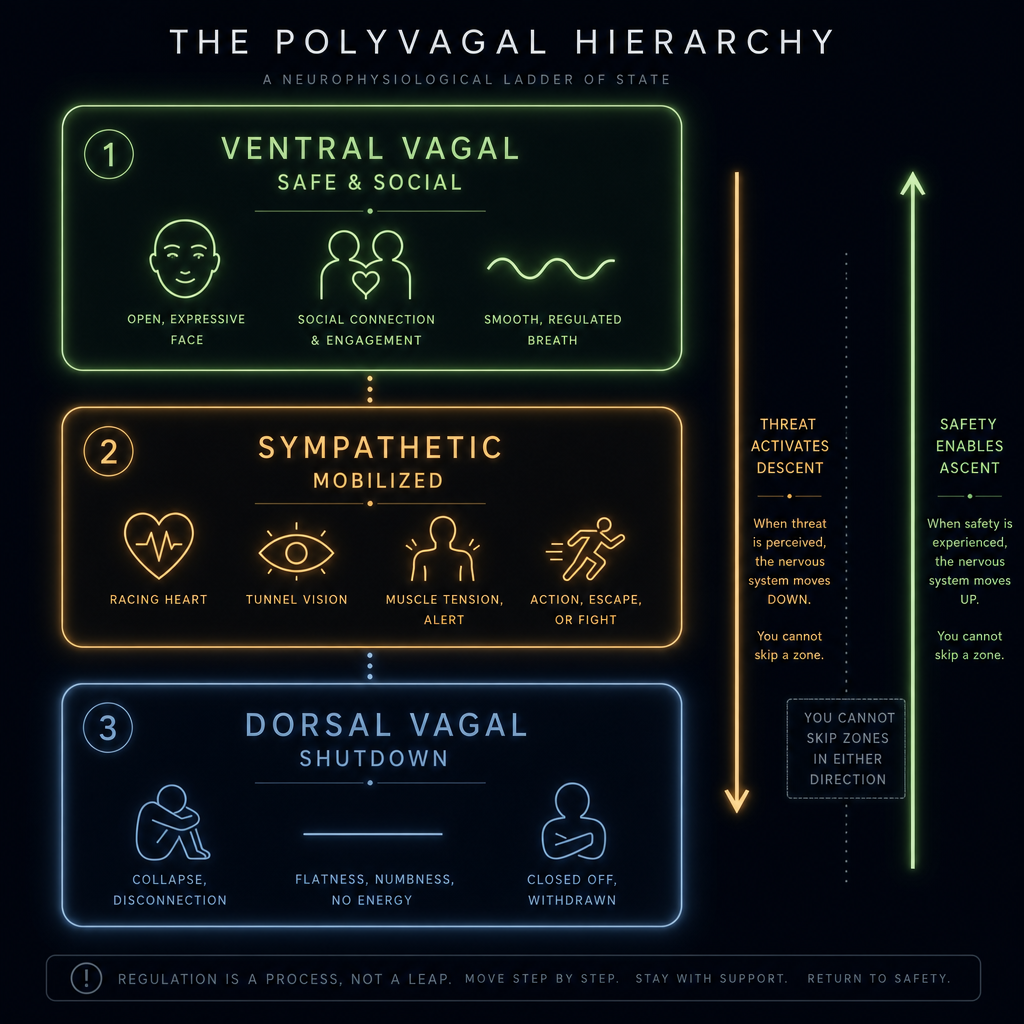
The nervous system has three distinct operating modes, organized by evolutionary age. Under threat, the system descends through them in order. Under safety, it ascends.
Ventral Vagal: Safe and Social
The newest and most evolutionarily recent system. Unique to mammals. Governs the social engagement system: facial expression, vocal prosody (the tonal quality of voice), head turning, listening, eye contact.
When ventral vagal is dominant:
- The face is expressive and readable
- The voice has range and warmth
- The body is open and accessible
- Thinking is broad, relational, creative
- Connection is possible and rewarding
This is the state from which learning, habit change, and genuine relationship all happen. The brain map can update here. Choices are available here. New pathways can be built here.
Sympathetic: Mobilized
The middle layer. Evolutionarily older. The fight/flight system — designed to mobilize the body for action under genuine threat.
When sympathetic is dominant:
- Heart rate elevates, breathing shallows and quickens
- Peripheral vision narrows into tunnel vision
- Glucose floods the bloodstream
- The social engagement system goes offline — face becomes flat, voice loses warmth, listening degrades
- The body is preparing to run or fight, not to reflect or connect
This state is adaptive for physical danger. It becomes costly when it runs chronically in response to social, relational, or psychological threat — which it was not designed to handle.
Dorsal Vagal: Shutdown
The oldest layer. The system of last resort when mobilization has failed or threat is inescapable. Found in all vertebrates — the playing-dead response in prey animals.
When dorsal vagal is dominant:
- Heart rate drops, breathing slows and shallows
- Numbness, dissociation, emotional flatness
- The impulse to move collapses
- The world recedes; internal experience dims
- Nothing feels possible or worth attempting
Dorsal vagal is not rest. It is collapse. From the outside it can look like calm — quiet, still, low-energy — but the inner experience is the opposite: not peaceful but absent. Not safe but unreachable.
The Hierarchy Is Not Random
The zones are not interchangeable. Under threat, the system descends in order: ventral → sympathetic → dorsal. It does not skip levels. Under safety, it ascends the same way.
This has direct consequences:
You cannot move directly from dorsal vagal to ventral vagal. Freeze does not lift into warmth and connection. It lifts first into anxiety, irritability, and restlessness — sympathetic activation — before it can ascend to safety. That is not a relapse. That is the correct direction.
The tools that work in sympathetic are the wrong tools for dorsal. Trying to calm down when you’re in freeze makes it worse — the system needs gentle activation, not further quieting. Trying to activate when you’re flooding makes it worse — the system needs discharge, not more input. The zone you’re in determines which tools can work.
In dorsal vagal, the habit layer is offline. The cortex is partially disconnected from executive function. Asking for conscious habit choices from shutdown is asking the brain to do something it cannot do at that moment — not because of weakness, but because the architecture is not available. The intervention in dorsal is not habit work. It is ascent.
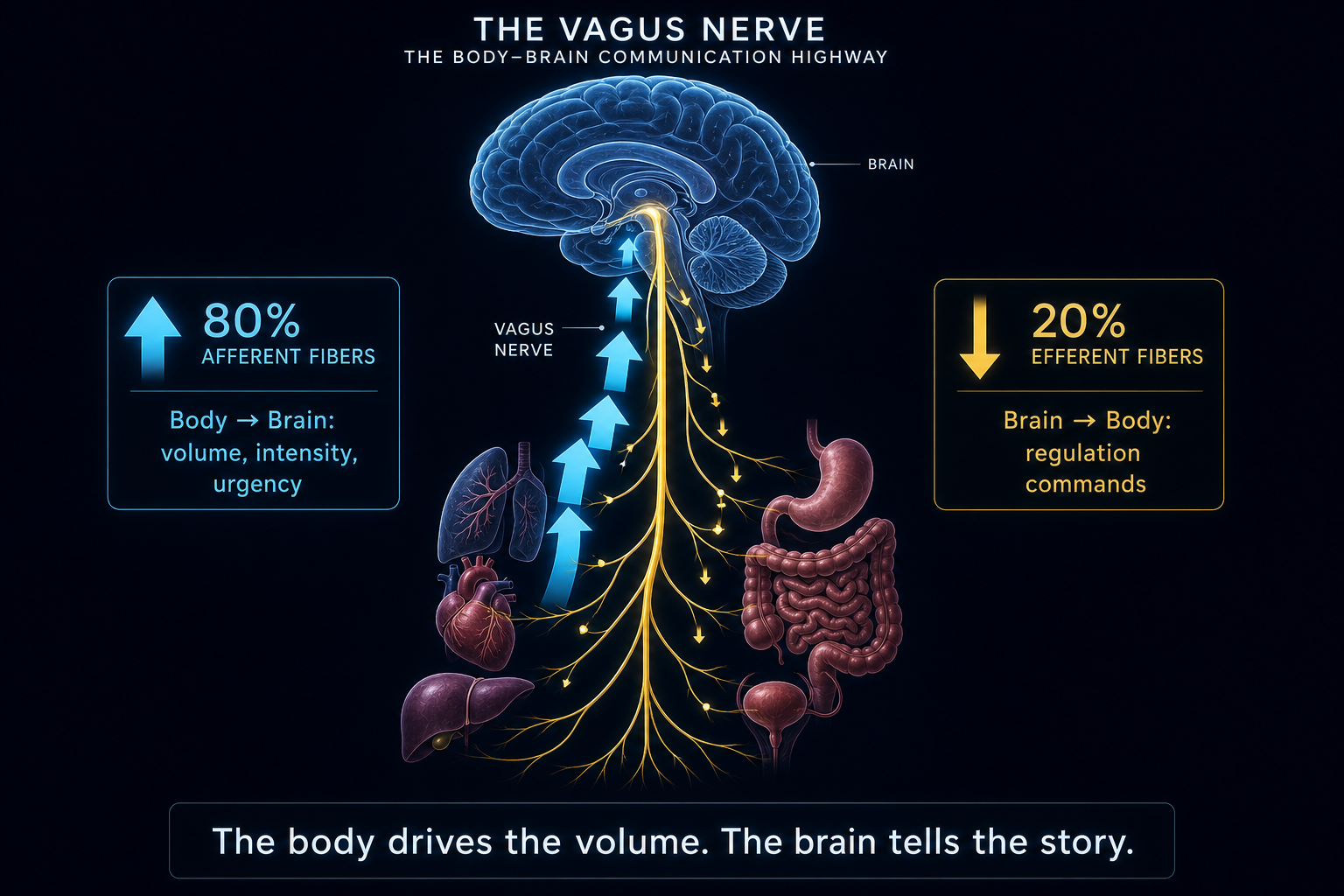
The 80% Afferent Fact
80% of vagus nerve fibers run afferent — from body to brain, not brain to body.
This is the most counterintuitive and most important fact in the whole model. Your emotional experience is mostly your body reporting to your brain, not your brain generating a response to external events.
The volume, the urgency, the intensity of what you feel — these are body signals. The brain receives them and builds a narrative around them. The narrative feels like the cause. It is largely the consequence.
This is why:
- Thinking harder about your feelings often makes them louder — you’re adding narrative to an already-running body process, which amplifies it
- Changing your breath immediately changes your emotional state — the afferent signal shifts before the story has time to catch up
- Eating something substantial when dysregulated often resolves what felt like a psychological problem — the metabolic signal was driving the distress
- Movement completes nervous system cycles that reflection cannot — because the cycle lives in the body, not the cognition
The path to regulation runs through the body. The mind can accompany it. It cannot lead.
Nervous System Cycles
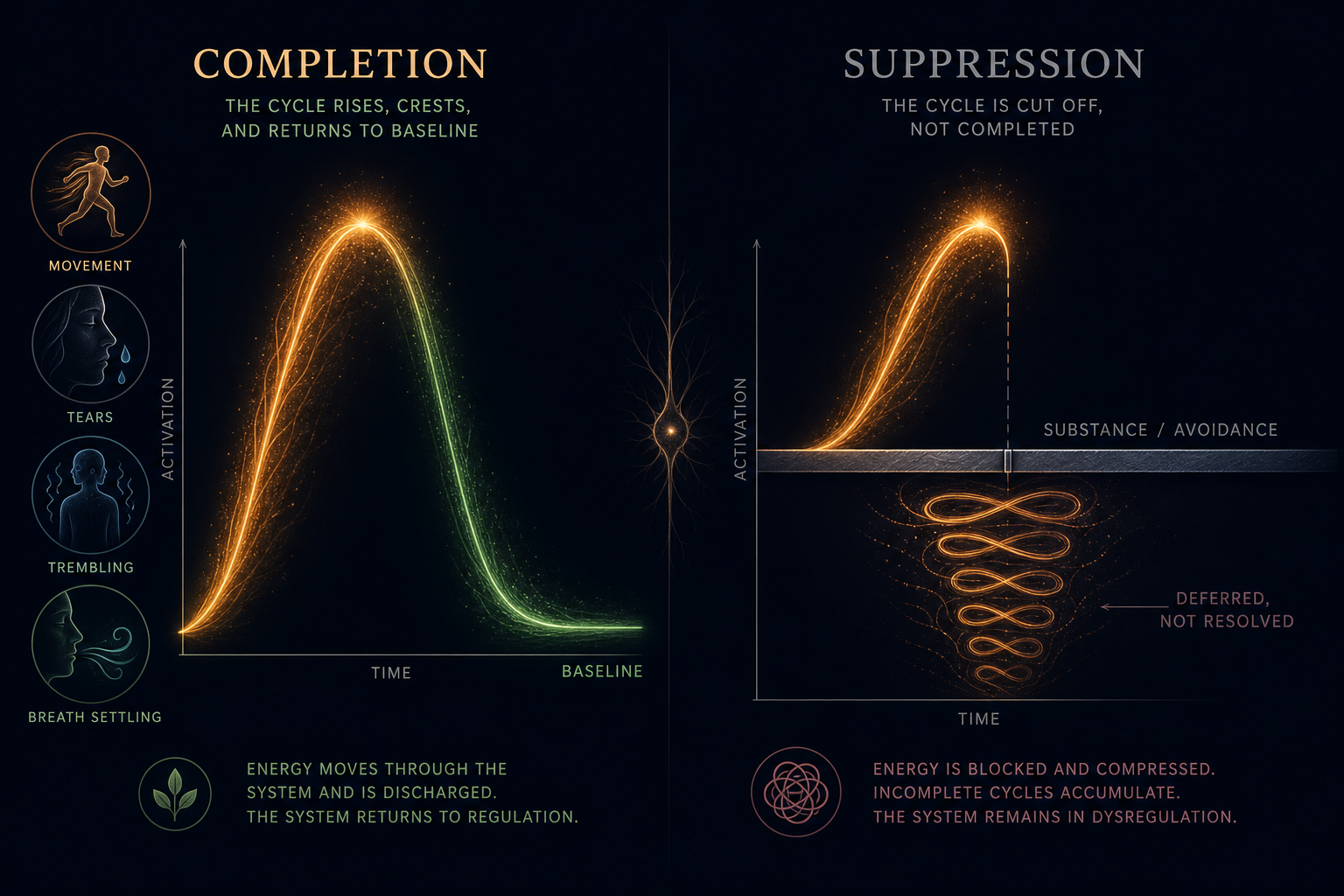
Every nervous system activation is a cycle with a beginning, a middle, and an end. Fear, grief, anger, longing, excitement — each is a wave that rises, peaks, and can complete.
The end of a cycle is not the resolution of the external situation. It is the physiological discharge: the trembling that releases, the crying that finishes, the breath that settles, the warmth that returns. The cycle completes in the body, independently of whether the external problem was solved.
Substances, avoidance, and distraction interrupt cycles before they complete. The cycle is deferred, not resolved. The backlog accumulates.
When suppression is removed — when the substance stops, when avoidance is no longer working — the backlog surfaces. This presents as intense emotion with no clear current cause: grief that feels disproportionate, crying with no obvious reason, waves of feeling that come and go over 20–40 minutes. This is not regression. This is the system completing what it started. Completed cycles are the biological substrate of recovery. Deferred cycles are the biological substrate of chronic dysregulation.
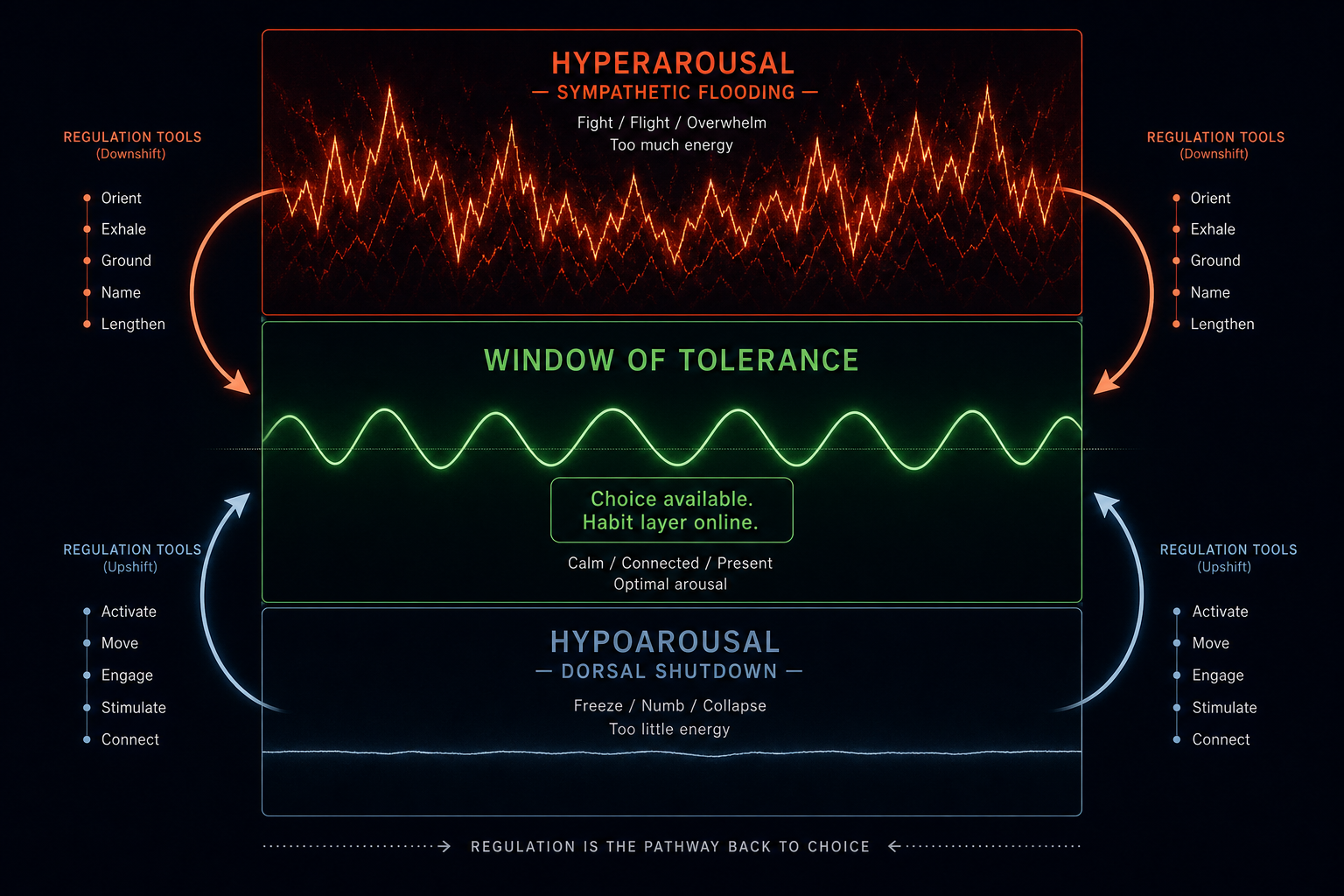
The Window of Tolerance
Between full sympathetic flooding and dorsal shutdown, there is a zone where the cortex remains online and regulation is possible. This is the window of tolerance.
Inside the window:
- Emotions are felt without being overwhelming
- Reflection is possible alongside sensation
- Choice is accessible
- New pathways can be laid; the habit layer can update
Outside the window — whether above it (sympathetic flooding) or below it (dorsal collapse):
- Cortical access is reduced or absent
- Reflection loops back into activation rather than resolving it
- Choice collapses into pattern execution
- The habit layer freezes
Most regulation work happens at the edge of the window — using somatic tools to bring the system back into range before cognitive work is attempted. This is why the app always regulates first, reflects later. Not as protocol. As architecture.
The 22 States and Polyvagal Zones
The 22 named nervous system states cluster strongly by polyvagal zone — because your zone is a primary determinant of which states are reachable at all.
Ventral vagal region — the states where habit change is possible, where new pathways can be built, where the brain map can update: Parasympathetic Rest, Baseline Maintenance, Orientation/Re-entry, Focused Attention, Social Engagement, Assertive Boundary, Curiosity/Inquiry, Play/Improvisation, Satiation/Completion, Existential Neutrality, Integration/Meaning-Making.
Sympathetic region — activated, mobilized. Some states here are highly functional (SEEKING, Flow, Performance at moderate intensity). Others are costly. All require discharge or transition to ventral to be sustainable: SEEKING/Desire, Flow/Effortless Action, Performance/Pressure, Anxiety/Hypervigilance, Fight/Anger Mobilization.
Dorsal vagal region — collapsed, offline. The primary intervention in these states is not habit work. It is activation: gentle movement, metabolic support, sensory re-engagement. The ascent through sympathetic must happen before the ascent to ventral can begin: Sleep, Freeze/Shutdown, Depressive/Low-Energy.
What Moves You Between Zones
Polyvagal zone is not fixed. It is influenced — most directly by:
Breath — the fastest voluntary lever. Lengthening the exhale activates the vagal brake via respiratory sinus arrhythmia. This is why breathing changes emotional state faster than any cognitive intervention.
Voice and sound — humming, singing, and gargling directly stimulate the vagus nerve through branches in the larynx and pharynx. The social engagement system (voice, face, listening) and the ventral vagal branch are architecturally tightly coupled.
Movement — physical exertion completes sympathetic cycles by processing the mobilization energy the body prepared. Gentle movement activates a collapsed system upward from dorsal. The type matters: intense exercise from sympathetic activation completes cycles; gentle movement from dorsal initiates ascent.
Metabolic state — hunger, depletion, substance interference, and sleep debt all directly affect polyvagal zone. A nervous system running on inadequate fuel defaults toward dorsal regardless of intention. A well-fueled system has more range and recovers faster.
Co-regulation — a regulated nervous system transmits safety to a dysregulated one through voice prosody, facial expression, and touch. Oxytocin released by safe social contact directly modulates vagal tone. This is why human presence is one of the most powerful regulation tools, and why isolation is so corrosive.
Temperature — cold water on the face activates the diving reflex and can interrupt acute sympathetic flooding. Warmth supports ventral tone.